



















よむ、つかう、まなぶ。
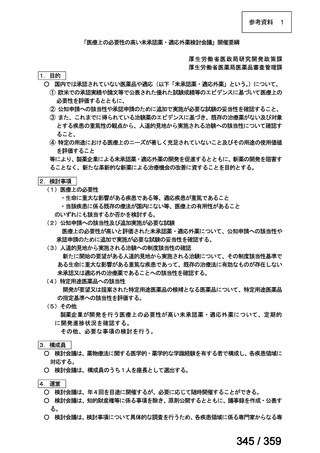
会議資料 (57 ページ)
出典
| 公開元URL | https://www.mhlw.go.jp/stf/shingi2/0000198856_00042.html |
| 出典情報 | 医薬・生活衛生局が実施する検討会 医療上の必要性の高い未承認薬・適応外薬検討会議(第64回 7/4)《厚生労働省》 |
ページ画像
ダウンロードした画像を利用する際は「出典情報」を明記してください。
低解像度画像をダウンロード
プレーンテキスト
資料テキストはコンピュータによる自動処理で生成されており、完全に資料と一致しない場合があります。
テキストをコピーしてご利用いただく際は資料と付け合わせてご確認ください。
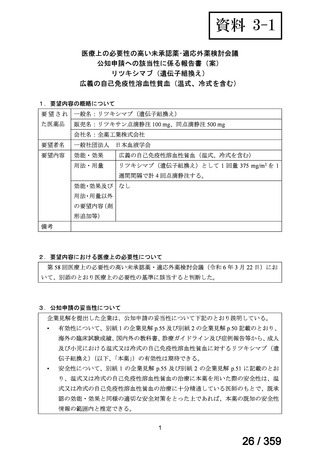
(公知申請への該当性に係る企業見解の様式)
要望番号;IV-168
Patients should be advised to avoid cold exposure where possible (1C)
Indications
for treatment: symptomatic anaemia, severe circulatory
symptoms or transfusion dependence (1C)
First line treatment: rituximab, or if clonality has been demonstrated,
the addition of fludarabine may be considered (1B)
特発性 CAD に対する治療
可能な限り寒冷曝露を避ける(1C)
治療の適応:症候性の貧血、重篤な循環器症状、輸血依存症(1C)
ファーストライン治療:リツキシマブ、又はクローナルな増殖が
認められる場合はフルダラビンの追加を考慮する(1B)
4. Childhood AIHA
Management
The management of AIHA in children is similar to that described in the
adult sections above.…(中略)…The best-studied second line agent is
rituximab, with response rates of 75-100% in children with primary or
secondary AIHA.
小児 AIHA
管理
小児 AIHA の管理は、成人の場合と同様である。…(中略)…最も
研究されているセカンドライン治療薬はリツキシマブであり、小児
の原発性又は続発性 AIHA における本剤の奏効率は 75~100%であ
る。
(下線部は要望内容に係る部分)
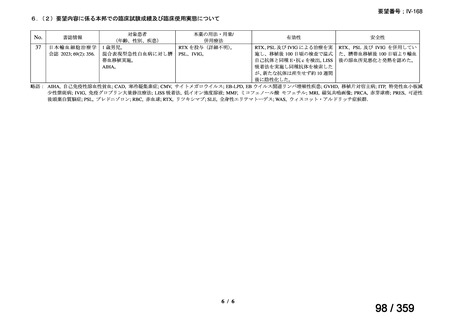
用法・用量
Specific management strategies
(または用法・用量に関
1. Primary warm AIHA - second line treatment: Recommendation
連のある記載箇所)
Rituximab
The standard regimen is 375 mg/m2 weekly for four consecutive weeks
but low dose rituximab achieves profound B cell suppression when used
for autoimmune disorders (Provan et al, 2007). Rituximab 100mg
weekly for 4 weeks with prednisolone, first or second line (Barcellini et
al, 2012), produced comparable response rates. However, rituximab was
used at an earlier disease stage than studies of standard dose therapy, and
variable definitions of response and short follow-up further limit
comparison.
具体的な管理戦略
特発性温式 AIHA に対するセカンドライン治療
28
57 / 359
要望番号;IV-168
Patients should be advised to avoid cold exposure where possible (1C)
Indications
for treatment: symptomatic anaemia, severe circulatory
symptoms or transfusion dependence (1C)
First line treatment: rituximab, or if clonality has been demonstrated,
the addition of fludarabine may be considered (1B)
特発性 CAD に対する治療
可能な限り寒冷曝露を避ける(1C)
治療の適応:症候性の貧血、重篤な循環器症状、輸血依存症(1C)
ファーストライン治療:リツキシマブ、又はクローナルな増殖が
認められる場合はフルダラビンの追加を考慮する(1B)
4. Childhood AIHA
Management
The management of AIHA in children is similar to that described in the
adult sections above.…(中略)…The best-studied second line agent is
rituximab, with response rates of 75-100% in children with primary or
secondary AIHA.
小児 AIHA
管理
小児 AIHA の管理は、成人の場合と同様である。…(中略)…最も
研究されているセカンドライン治療薬はリツキシマブであり、小児
の原発性又は続発性 AIHA における本剤の奏効率は 75~100%であ
る。
(下線部は要望内容に係る部分)
用法・用量
Specific management strategies
(または用法・用量に関
1. Primary warm AIHA - second line treatment: Recommendation
連のある記載箇所)
Rituximab
The standard regimen is 375 mg/m2 weekly for four consecutive weeks
but low dose rituximab achieves profound B cell suppression when used
for autoimmune disorders (Provan et al, 2007). Rituximab 100mg
weekly for 4 weeks with prednisolone, first or second line (Barcellini et
al, 2012), produced comparable response rates. However, rituximab was
used at an earlier disease stage than studies of standard dose therapy, and
variable definitions of response and short follow-up further limit
comparison.
具体的な管理戦略
特発性温式 AIHA に対するセカンドライン治療
28
57 / 359