





























よむ、つかう、まなぶ。
資料5-1 Ⅳ-203 モキシフロキサシン塩酸塩[15.1MB] (114 ページ)
出典
| 公開元URL | https://www.mhlw.go.jp/stf/shingi2/0000198856_00044.html |
| 出典情報 | 医療上の必要性の高い未承認薬・適応外薬検討会議(第66回 12/12)《厚生労働省》 |
ページ画像
ダウンロードした画像を利用する際は「出典情報」を明記してください。
低解像度画像をダウンロード
プレーンテキスト
資料テキストはコンピュータによる自動処理で生成されており、完全に資料と一致しない場合があります。
テキストをコピーしてご利用いただく際は資料と付け合わせてご確認ください。
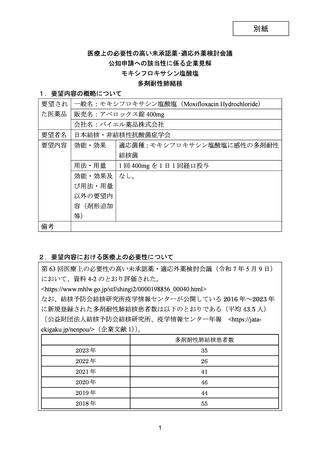
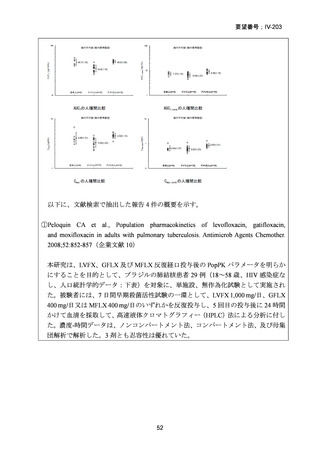
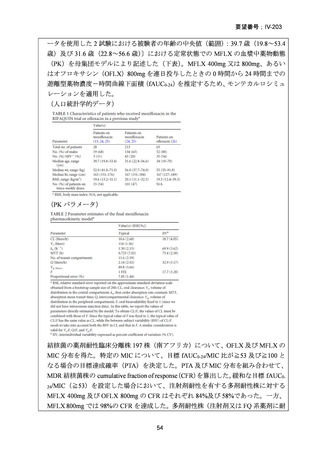
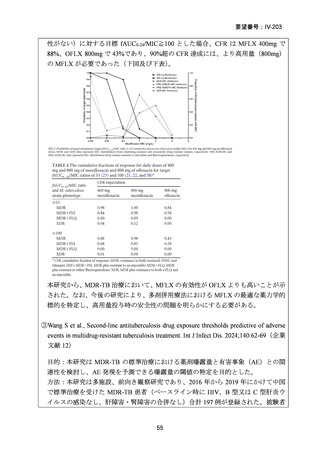
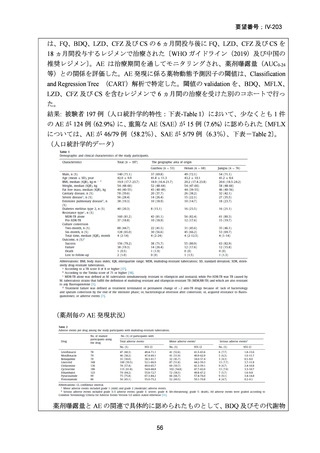
要望番号;IV-203
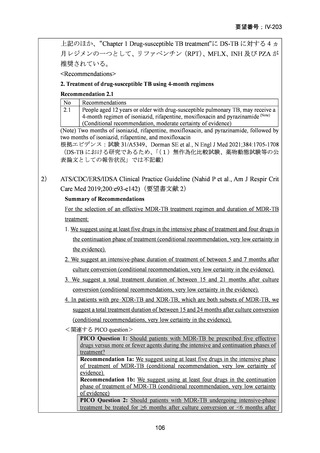
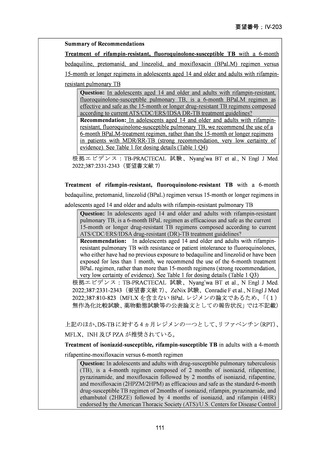
PICO Question 20b: Should patients with isoniazid-resistant TB be treated with a
regimen composed of fluoroquinolone, rifampin, and ethambutol for 6 months and
pyrazinamide for the first 2 months compared with a regimen composed of a
fluoroquinolone, rifampin, ethambutol, and pyrazinamide for 6 months?
Recommendation 20a: We suggest adding a later-generation fluoroquinolone to a
6-month regimen of daily rifampin, ethambutol, and pyrazinamide for patients with
isoniazid-resistant TB (conditional recommendation, very low certainty in the
evidence).
Recommendation 20b: In patients with isoniazid-resistant TB treated with a daily
regimen of a later-generation fluoroquinolone, rifampin, ethambutol, and
pyrazinamide, we suggest that the duration of pyrazinamide can be shortened to
2 months in selected situations (i.e., noncavitary and lower-burden disease or
toxicity from pyrazinamide) (conditional recommendation, very low certainty in the
evidence)
根拠エビデンス:Fregonese F et al., Lancet Respir Med 2018;6:265-275(INH-R TB の治療
レジメンの論文であるため、
「
(1)無作為化比較試験、薬物動態試験等の公表論文と
しての報告状況」では不記載)
For the management of contacts to patients with MDR-TB:
25. We suggest offering treatment for latent TB infection (LTBI) for contacts to patients
with MDR-TB versus following with observation alone (conditional recommendation,
very low certainty in the evidence).
We suggest 6 to 12 months of treatment with a later-generation fluoroquinolone alone
or with a second drug, on the basis of drug susceptibility of the source-case M.
tuberculosis isolate. On the basis of evidence of increased toxicity, adverse events, and
discontinuations, pyrazinamide should not be routinely used as the second drug.
<関連する PICO question>
PICO Question 21: Treatment of Contacts Exposed to MDR-TB: Should contacts
exposed to an infectious patient with MDR-TB be offered LTBI treatment versus
followed with observation alone?
Recommendation 21: For contacts with presumed MDR LTBI due to exposure to
an infectious patient with MDR-TB, we suggest offering treatment for LTBI
(conditional recommendation, very low certainty in the evidence). We suggest 6 to
12 months of treatment with a later-generation fluoroquinolone alone or with a
second drug, on the basis of drug susceptibility of the source-case M. tuberculosis
isolate. On the basis of evidence of increased toxicity, adverse events, and
discontinuations, pyrazinamide should not be routinely used as the second drug.
根拠エビデンス:Marks SM et al., Clin Infect Dis 2017;64:1670-1677
(予防的使用の研究であり、MFLX と LVFX の使用割合も明らかでないため、
「(1)無作為化比較試験、薬物動態試験等の公表論文としての報告状況」では
不記載)
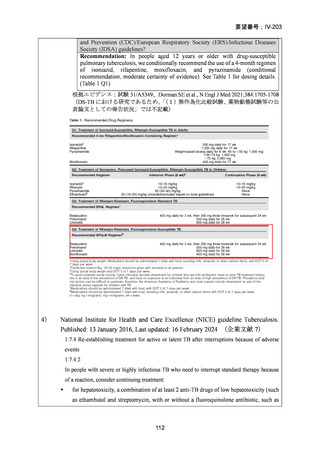
3)
Updates on the treatment of drug-susceptible and drug-resistant tuberculosis, An
official ATS/CDC/ERS/IDSA Clinical Practice Guideline (Saukkonen JJ et al., Am J
Respir Crit Care Med 2025;211:15-33)(企業文献 3)
110
PICO Question 20b: Should patients with isoniazid-resistant TB be treated with a
regimen composed of fluoroquinolone, rifampin, and ethambutol for 6 months and
pyrazinamide for the first 2 months compared with a regimen composed of a
fluoroquinolone, rifampin, ethambutol, and pyrazinamide for 6 months?
Recommendation 20a: We suggest adding a later-generation fluoroquinolone to a
6-month regimen of daily rifampin, ethambutol, and pyrazinamide for patients with
isoniazid-resistant TB (conditional recommendation, very low certainty in the
evidence).
Recommendation 20b: In patients with isoniazid-resistant TB treated with a daily
regimen of a later-generation fluoroquinolone, rifampin, ethambutol, and
pyrazinamide, we suggest that the duration of pyrazinamide can be shortened to
2 months in selected situations (i.e., noncavitary and lower-burden disease or
toxicity from pyrazinamide) (conditional recommendation, very low certainty in the
evidence)
根拠エビデンス:Fregonese F et al., Lancet Respir Med 2018;6:265-275(INH-R TB の治療
レジメンの論文であるため、
「
(1)無作為化比較試験、薬物動態試験等の公表論文と
しての報告状況」では不記載)
For the management of contacts to patients with MDR-TB:
25. We suggest offering treatment for latent TB infection (LTBI) for contacts to patients
with MDR-TB versus following with observation alone (conditional recommendation,
very low certainty in the evidence).
We suggest 6 to 12 months of treatment with a later-generation fluoroquinolone alone
or with a second drug, on the basis of drug susceptibility of the source-case M.
tuberculosis isolate. On the basis of evidence of increased toxicity, adverse events, and
discontinuations, pyrazinamide should not be routinely used as the second drug.
<関連する PICO question>
PICO Question 21: Treatment of Contacts Exposed to MDR-TB: Should contacts
exposed to an infectious patient with MDR-TB be offered LTBI treatment versus
followed with observation alone?
Recommendation 21: For contacts with presumed MDR LTBI due to exposure to
an infectious patient with MDR-TB, we suggest offering treatment for LTBI
(conditional recommendation, very low certainty in the evidence). We suggest 6 to
12 months of treatment with a later-generation fluoroquinolone alone or with a
second drug, on the basis of drug susceptibility of the source-case M. tuberculosis
isolate. On the basis of evidence of increased toxicity, adverse events, and
discontinuations, pyrazinamide should not be routinely used as the second drug.
根拠エビデンス:Marks SM et al., Clin Infect Dis 2017;64:1670-1677
(予防的使用の研究であり、MFLX と LVFX の使用割合も明らかでないため、
「(1)無作為化比較試験、薬物動態試験等の公表論文としての報告状況」では
不記載)
3)
Updates on the treatment of drug-susceptible and drug-resistant tuberculosis, An
official ATS/CDC/ERS/IDSA Clinical Practice Guideline (Saukkonen JJ et al., Am J
Respir Crit Care Med 2025;211:15-33)(企業文献 3)
110