









よむ、つかう、まなぶ。
資料3-6 コルヒチンの安全対策のための製造販売承認事項一部変更承認について[1.7MB] (15 ページ)
出典
| 公開元URL | https://www.mhlw.go.jp/stf/newpage_73884.html |
| 出典情報 | 薬事審議会 医薬品等安全対策部会(令和8年度第1回 6/18)《厚生労働省》 |
ページ画像
ダウンロードした画像を利用する際は「出典情報」を明記してください。
低解像度画像をダウンロード
プレーンテキスト
資料テキストはコンピュータによる自動処理で生成されており、完全に資料と一致しない場合があります。
テキストをコピーしてご利用いただく際は資料と付け合わせてご確認ください。
COLCHICINE FOR EARLY ACUTE GOUT FLARE
1063
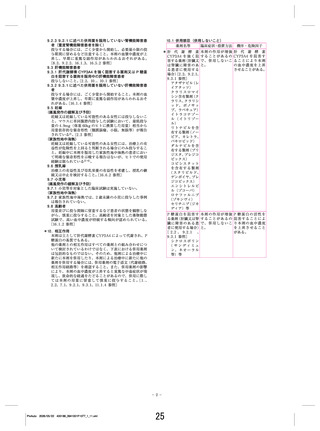
Table 1. Baseline characteristics of the patients (safety population, n ⫽ 185)*
Demographics
Age, mean ⫾ SD years
Men
Race
American Indian/Alaska Native
Asian
Black/African American
White/Caucasian
Other
History of gout
Age at onset, mean ⫾ SD years
Attacks in the year prior to screening, mean ⫾ SD
Time since most recent flare, mean ⫾ SD months
Urate concentration, mean ⫾ SD mg/dl
Concurrent allopurinol use
Presence of ⱖ1 tophi
Previously met ACR preliminary criteria for acute gout
Body weight, mean ⫾ SD lb
BMI, mean ⫾ SD kg/m2
High-dose
colchicine
(n ⫽ 52)
Low-dose
colchicine
(n ⫽ 74)
Placebo
(n ⫽ 59)
Overall
(n ⫽ 185)
51.9 ⫾ 10.02
49 (94.2)
51.4 ⫾ 11.79
72 (97.3)
51.2 ⫾ 11.36
55 (93.2)
51.5 ⫾ 11.12
176 (95.1)
0 (0)
0 (0)
10 (19.2)
40 (76.9)
2 (3.8)
1 (1.4)
1 (1.4)
4 (5.4)
66 (89.2)
2 (2.7)
0 (0)
1 (1.7)
11 (18.6)
47 (79.7)
0 (0)
1 (0.5)
2 (1.1)
25 (13.5)
153 (82.7)
4 (2.2)
40.7 ⫾ 11.83
4.7 ⫾ 3.28
1.4 ⫾ 1.44
9.2 ⫾ 1.7
10 (19.2)
7 (14)
52 (100)
228 ⫾ 38.10
32.9 ⫾ 4.63
40.7 ⫾ 12.38
4.4 ⫾ 2.24
1.6 ⫾ 1.36
8.5 ⫾ 1.8
29 (39.2)
5 (7)
74 (100)
228 ⫾ 42.44
33.2 ⫾ 6.27
41.6 ⫾ 13.20
3.8 ⫾ 2.02
1.7 ⫾ 1.84
8.9 ⫾ 1.9
15 (25.4)
5 (9)
59 (100)
228 ⫾ 41.69
32.8 ⫾ 5.82
41.0 ⫾ 12.44
4.3 ⫾ 2.52
1.6 ⫾ 1.55
8.8 ⫾ 1.8
54 (29.2)
17 (9)
185 (100)
228 ⫾ 40.80
33.0 ⫾ 5.68
* Except where indicated otherwise, values are the number (%) of patients. ACR ⫽ American College of Rheumatology; BMI ⫽ body mass index.
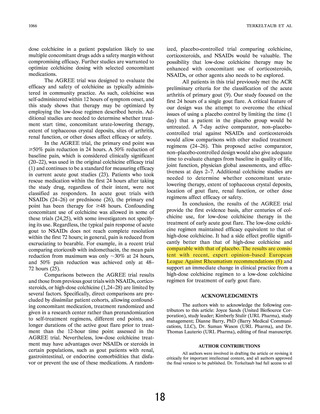
patients received placebo. All but 1 patient (n ⫽ 184)
had a flare confirmed by the Gout Flare Call Center
(intent-to-treat population) (Figure 2). Demographic
and gout characteristics were similar among the 3 treatment groups. The majority of patients were overweight
white men ⬃50 years of age with an elevated serum
urate concentration and a 10-year history of gout. Less
than one-third of patients were receiving concurrent
urate-lowering therapy at the start of the study. No
patient started or altered urate-lowering therapy during
the study. Tophi were present in ⬃9% of patients (Table
1). According to investigator assessment, 94.6% of patients were compliant with taking their study medication.
Findings of the AGREE efficacy evaluation. Both
colchicine regimens were significantly more effective
than placebo, with 17 responders (32.7%) in the highdose group, 28 responders (37.8%) in the low-dose
group, and 9 responders (15.5%) in the placebo group
(P ⫽ 0.034 and P ⫽ 0.005, respectively, versus placebo).
Alternate definitions of response were declared a priori
secondary outcome measures (Table 2). The percent of
responding patients was proportionally greater in the
low-dose group compared with that in the high-dose and
placebo groups across the entire pain improvement
range (Figure 3).
Most rescue medications used in this trial were
NSAIDs, with indomethacin predominating. Rescue
medication was taken within the first 24 hours by 23
patients (31.1%) in the low-dose colchicine group, 18
patients (34.6%) in the high-dose colchicine group, and
29 patients (50.0%) in the placebo group. These patients
were considered nonresponders. Compared with patients receiving placebo, significantly fewer patients in
the low-dose colchicine group (odds ratio [OR] 0.45
[95% CI 0.22–0.92], P ⫽ 0.027) took rescue medication
prior to hour 24. Fewer patients in the high-dose colchicine group than in the placebo group (OR 0.53 [95% CI
0.25–1.14]) took rescue medication prior to hour 24,
although the difference did not reach statistical significance (P ⫽ 0.103).
The computation of the OR (95% CI) for confounding bias did not detect differences in any of the
prespecified parameters that included demographics
(age, sex, or race) or other baseline characteristics
(concomitant use of allopurinol or diuretics, time since
first diagnosis of gout, number of flares within the past
12 months, or alcohol use) associated with the proportion of patients who met response criteria at 24 hours.
Although serum urate levels chosen a priori (ⱕ7 versus
⬎7 mg/dl) showed no confounding bias, post hoc exploratory analysis showed that patients with a serum urate
level ⬎10.0 mg/dl at screening were less likely to be
responders compared with patients with a serum urate
level ⱕ10 mg/dl (OR 0.29 [95% CI 0.12–0.74]).
Findings of the AGREE safety evaluation. There
were no deaths, serious AEs, or patient withdrawals due
to AEs in this study. All AEs in the low-dose group were
mild to moderate in intensity, while 19.2% of the
15
1063
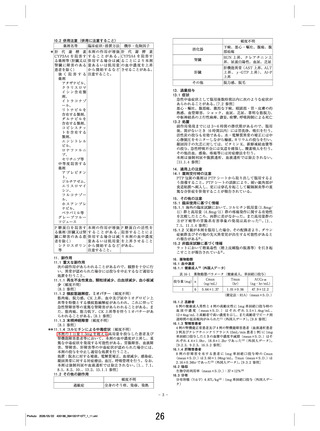
Table 1. Baseline characteristics of the patients (safety population, n ⫽ 185)*
Demographics
Age, mean ⫾ SD years
Men
Race
American Indian/Alaska Native
Asian
Black/African American
White/Caucasian
Other
History of gout
Age at onset, mean ⫾ SD years
Attacks in the year prior to screening, mean ⫾ SD
Time since most recent flare, mean ⫾ SD months
Urate concentration, mean ⫾ SD mg/dl
Concurrent allopurinol use
Presence of ⱖ1 tophi
Previously met ACR preliminary criteria for acute gout
Body weight, mean ⫾ SD lb
BMI, mean ⫾ SD kg/m2
High-dose
colchicine
(n ⫽ 52)
Low-dose
colchicine
(n ⫽ 74)
Placebo
(n ⫽ 59)
Overall
(n ⫽ 185)
51.9 ⫾ 10.02
49 (94.2)
51.4 ⫾ 11.79
72 (97.3)
51.2 ⫾ 11.36
55 (93.2)
51.5 ⫾ 11.12
176 (95.1)
0 (0)
0 (0)
10 (19.2)
40 (76.9)
2 (3.8)
1 (1.4)
1 (1.4)
4 (5.4)
66 (89.2)
2 (2.7)
0 (0)
1 (1.7)
11 (18.6)
47 (79.7)
0 (0)
1 (0.5)
2 (1.1)
25 (13.5)
153 (82.7)
4 (2.2)
40.7 ⫾ 11.83
4.7 ⫾ 3.28
1.4 ⫾ 1.44
9.2 ⫾ 1.7
10 (19.2)
7 (14)
52 (100)
228 ⫾ 38.10
32.9 ⫾ 4.63
40.7 ⫾ 12.38
4.4 ⫾ 2.24
1.6 ⫾ 1.36
8.5 ⫾ 1.8
29 (39.2)
5 (7)
74 (100)
228 ⫾ 42.44
33.2 ⫾ 6.27
41.6 ⫾ 13.20
3.8 ⫾ 2.02
1.7 ⫾ 1.84
8.9 ⫾ 1.9
15 (25.4)
5 (9)
59 (100)
228 ⫾ 41.69
32.8 ⫾ 5.82
41.0 ⫾ 12.44
4.3 ⫾ 2.52
1.6 ⫾ 1.55
8.8 ⫾ 1.8
54 (29.2)
17 (9)
185 (100)
228 ⫾ 40.80
33.0 ⫾ 5.68
* Except where indicated otherwise, values are the number (%) of patients. ACR ⫽ American College of Rheumatology; BMI ⫽ body mass index.
patients received placebo. All but 1 patient (n ⫽ 184)
had a flare confirmed by the Gout Flare Call Center
(intent-to-treat population) (Figure 2). Demographic
and gout characteristics were similar among the 3 treatment groups. The majority of patients were overweight
white men ⬃50 years of age with an elevated serum
urate concentration and a 10-year history of gout. Less
than one-third of patients were receiving concurrent
urate-lowering therapy at the start of the study. No
patient started or altered urate-lowering therapy during
the study. Tophi were present in ⬃9% of patients (Table
1). According to investigator assessment, 94.6% of patients were compliant with taking their study medication.
Findings of the AGREE efficacy evaluation. Both
colchicine regimens were significantly more effective
than placebo, with 17 responders (32.7%) in the highdose group, 28 responders (37.8%) in the low-dose
group, and 9 responders (15.5%) in the placebo group
(P ⫽ 0.034 and P ⫽ 0.005, respectively, versus placebo).
Alternate definitions of response were declared a priori
secondary outcome measures (Table 2). The percent of
responding patients was proportionally greater in the
low-dose group compared with that in the high-dose and
placebo groups across the entire pain improvement
range (Figure 3).
Most rescue medications used in this trial were
NSAIDs, with indomethacin predominating. Rescue
medication was taken within the first 24 hours by 23
patients (31.1%) in the low-dose colchicine group, 18
patients (34.6%) in the high-dose colchicine group, and
29 patients (50.0%) in the placebo group. These patients
were considered nonresponders. Compared with patients receiving placebo, significantly fewer patients in
the low-dose colchicine group (odds ratio [OR] 0.45
[95% CI 0.22–0.92], P ⫽ 0.027) took rescue medication
prior to hour 24. Fewer patients in the high-dose colchicine group than in the placebo group (OR 0.53 [95% CI
0.25–1.14]) took rescue medication prior to hour 24,
although the difference did not reach statistical significance (P ⫽ 0.103).
The computation of the OR (95% CI) for confounding bias did not detect differences in any of the
prespecified parameters that included demographics
(age, sex, or race) or other baseline characteristics
(concomitant use of allopurinol or diuretics, time since
first diagnosis of gout, number of flares within the past
12 months, or alcohol use) associated with the proportion of patients who met response criteria at 24 hours.
Although serum urate levels chosen a priori (ⱕ7 versus
⬎7 mg/dl) showed no confounding bias, post hoc exploratory analysis showed that patients with a serum urate
level ⬎10.0 mg/dl at screening were less likely to be
responders compared with patients with a serum urate
level ⱕ10 mg/dl (OR 0.29 [95% CI 0.12–0.74]).
Findings of the AGREE safety evaluation. There
were no deaths, serious AEs, or patient withdrawals due
to AEs in this study. All AEs in the low-dose group were
mild to moderate in intensity, while 19.2% of the
15