









よむ、つかう、まなぶ。
資料3-6 コルヒチンの安全対策のための製造販売承認事項一部変更承認について[1.7MB] (13 ページ)
出典
| 公開元URL | https://www.mhlw.go.jp/stf/newpage_73884.html |
| 出典情報 | 薬事審議会 医薬品等安全対策部会(令和8年度第1回 6/18)《厚生労働省》 |
ページ画像
ダウンロードした画像を利用する際は「出典情報」を明記してください。
低解像度画像をダウンロード
プレーンテキスト
資料テキストはコンピュータによる自動処理で生成されており、完全に資料と一致しない場合があります。
テキストをコピーしてご利用いただく際は資料と付け合わせてご確認ください。
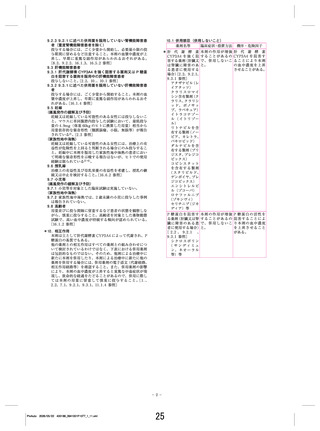
COLCHICINE FOR EARLY ACUTE GOUT FLARE
1061
with a safety profile indistinguishable from that of
placebo.
Colchicine is mainly used in the treatment and
prophylaxis of gout flare, although the evidence basis for
its use in treating acute gout flare remains remarkably
limited. Only 1 randomized, placebo-controlled trial
(n ⫽ 43) exploring colchicine in gout flare has previously
been reported (1). The regimen in that study was two
0.5-mg tablets followed by one tablet every 2 hours until
relief or marked toxicity (such as diarrhea, nausea, or
vomiting) occurred (1). Patients received a mean dose of
6.7 mg colchicine (1). Colchicine demonstrated statistical superiority over placebo in pain reduction in 48
hours, but diarrhea developed in 100% of colchicine
recipients by the time of clinical response (1).
High-dose (or prolonged) colchicine regimens,
such as the one described by Ahern et al (1), are
commonly prescribed for acute gout (2) despite a high
risk-to-benefit ratio (3–6). Lower-dose (or abbreviated)
regimens of colchicine have been suggested (5,7,8) but
never rigorously studied.
The AGREE (Acute Gout Flare Receiving Colchicine Evaluation) study compared low- and high-dose
colchicine using a randomized, placebo-controlled design. A list of clinical investigators in the AGREE trial is
provided in Appendix A. Pharmacokinetic profiles of the
high- and low-dose regimens were previously obtained in
healthy volunteers and demonstrated comparable maximum blood concentrations (C max ). The selfadministered high-dose prolonged colchicine regimen
(4.8 mg total over 6 hours) was selected to mimic
common practice (1,2) and was compared with a placebo
and a novel low-dose abbreviated regimen (1.8 mg total
over 1 hour). The results at the primary 24-hour end
point demonstrate superior safety of low-dose colchicine, without loss of efficacy, relative to high-dose
colchicine for early acute gout flare (self-administered
within 12 hours of flare onset).
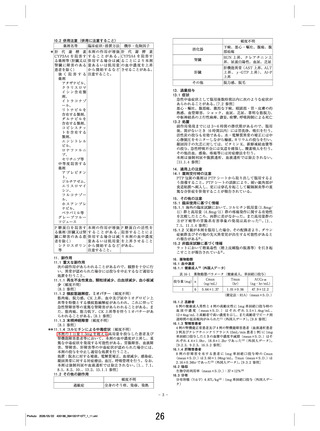
Figure 1. Pharmacokinetic properties of low-dose, high-dose, and
single-dose colchicine in healthy normal volunteers. Peak blood concentrations were similar in the low- and high-dose colchicine groups,
while total colchicine exposure (area under the curve from zero to
infinity) was proportional to the total colchicine dose received. Values
are the mean.
data from the samples were used to calculate Cmax, area under
the curve (AUC)0–⬁, and terminal half-life. Statistical analyses
were performed using WinNonlin software, version 5.0.1
(Pharsight, St. Louis, MO).
Peak blood levels (Cmax) for single-dose, low-dose, and
high-dose colchicine were 2.5, 6.19, and 6.84 ng/ml, respectively, in healthy volunteers, and exposure to colchicine
(AUC0–⬁) was 14.1, 52.1, and 118.2 nanograms ⫻ hours/ml,
respectively. The terminal half-lives for single-dose, low-dose,
and high-dose colchicine were 6.36, 23.6, and 31.4 hours,
respectively (Figure 1).
AGREE study population. Male and postmenopausal
female patients ⱖ18 years of age with a confirmed past
diagnosis of gout (according to the American College of
Rheumatology [ACR] classification criteria [9]) and having
had ⱖ2 gout flares within the prior 12 months were eligible for
randomization. A stable regimen of urate-lowering therapy
was permitted. A total of 575 patients were randomized to 1 of
3 treatment groups: 1) “low-dose” colchicine (1.2 mg followed
by 0.6 mg in 1 hour followed by placebo doses every hour for
5 hours [1.8 mg total]), 2) “high-dose” colchicine (1.2 mg
followed by 0.6 mg every hour for 6 hours [4.8 mg total]), or 3)
placebo (2 placebo capsules initially, followed by 1 placebo
capsule every hour for 6 hours).
AGREE study design. This was a multicenter, randomized, double-blind, placebo-controlled, parallel-group, dosecomparison study conducted between April 2007 and October
2008. A total of 54 centers in the US randomized and reported
at least 1 patient with a gout flare. Overencapsulated (to
preserve double-blindedness) colchicine (USP 0.6-mg tablets
[Colcrys]) and matching overencapsulated (to preserve
double-blindedness) placebo were provided by URL Pharma.
A key aspect of the study design was that patients were
enrolled and were dispensed a double-blinded blister card of
study medication, at screening, prior to the onset of a gout
flare. Patients were required to call the Gout Flare Call Center
before taking study medication. This center was staffed 24
hours a day by medically trained personnel (e.g., nurses). Upon
clearance from the Gout Flare Call Center, patients were
PATIENTS AND METHODS
Characterization of colchicine pharmacokinetics.
Prior to the AGREE trial, the pharmacokinetics of low-dose
colchicine (1.2 mg followed by 0.6 mg in 1 hour [1.8 mg total]),
“high-dose” colchicine (1.2 mg followed by 0.6 mg every hour
for 6 hours [4.8 mg total]), and single-dose (0.6 mg) colchicine
were evaluated in healthy volunteers who had fasted. None of
these healthy volunteers participated in the AGREE trial.
Colchicine, United States Pharmacopeia (USP) 0.6-mg tablets
(Colcrys), was provided by URL Pharma (Philadelphia, PA).
Pharmacokinetic sampling occurred over 96 hours. Analytic
13
1061
with a safety profile indistinguishable from that of
placebo.
Colchicine is mainly used in the treatment and
prophylaxis of gout flare, although the evidence basis for
its use in treating acute gout flare remains remarkably
limited. Only 1 randomized, placebo-controlled trial
(n ⫽ 43) exploring colchicine in gout flare has previously
been reported (1). The regimen in that study was two
0.5-mg tablets followed by one tablet every 2 hours until
relief or marked toxicity (such as diarrhea, nausea, or
vomiting) occurred (1). Patients received a mean dose of
6.7 mg colchicine (1). Colchicine demonstrated statistical superiority over placebo in pain reduction in 48
hours, but diarrhea developed in 100% of colchicine
recipients by the time of clinical response (1).
High-dose (or prolonged) colchicine regimens,
such as the one described by Ahern et al (1), are
commonly prescribed for acute gout (2) despite a high
risk-to-benefit ratio (3–6). Lower-dose (or abbreviated)
regimens of colchicine have been suggested (5,7,8) but
never rigorously studied.
The AGREE (Acute Gout Flare Receiving Colchicine Evaluation) study compared low- and high-dose
colchicine using a randomized, placebo-controlled design. A list of clinical investigators in the AGREE trial is
provided in Appendix A. Pharmacokinetic profiles of the
high- and low-dose regimens were previously obtained in
healthy volunteers and demonstrated comparable maximum blood concentrations (C max ). The selfadministered high-dose prolonged colchicine regimen
(4.8 mg total over 6 hours) was selected to mimic
common practice (1,2) and was compared with a placebo
and a novel low-dose abbreviated regimen (1.8 mg total
over 1 hour). The results at the primary 24-hour end
point demonstrate superior safety of low-dose colchicine, without loss of efficacy, relative to high-dose
colchicine for early acute gout flare (self-administered
within 12 hours of flare onset).
Figure 1. Pharmacokinetic properties of low-dose, high-dose, and
single-dose colchicine in healthy normal volunteers. Peak blood concentrations were similar in the low- and high-dose colchicine groups,
while total colchicine exposure (area under the curve from zero to
infinity) was proportional to the total colchicine dose received. Values
are the mean.
data from the samples were used to calculate Cmax, area under
the curve (AUC)0–⬁, and terminal half-life. Statistical analyses
were performed using WinNonlin software, version 5.0.1
(Pharsight, St. Louis, MO).
Peak blood levels (Cmax) for single-dose, low-dose, and
high-dose colchicine were 2.5, 6.19, and 6.84 ng/ml, respectively, in healthy volunteers, and exposure to colchicine
(AUC0–⬁) was 14.1, 52.1, and 118.2 nanograms ⫻ hours/ml,
respectively. The terminal half-lives for single-dose, low-dose,
and high-dose colchicine were 6.36, 23.6, and 31.4 hours,
respectively (Figure 1).
AGREE study population. Male and postmenopausal
female patients ⱖ18 years of age with a confirmed past
diagnosis of gout (according to the American College of
Rheumatology [ACR] classification criteria [9]) and having
had ⱖ2 gout flares within the prior 12 months were eligible for
randomization. A stable regimen of urate-lowering therapy
was permitted. A total of 575 patients were randomized to 1 of
3 treatment groups: 1) “low-dose” colchicine (1.2 mg followed
by 0.6 mg in 1 hour followed by placebo doses every hour for
5 hours [1.8 mg total]), 2) “high-dose” colchicine (1.2 mg
followed by 0.6 mg every hour for 6 hours [4.8 mg total]), or 3)
placebo (2 placebo capsules initially, followed by 1 placebo
capsule every hour for 6 hours).
AGREE study design. This was a multicenter, randomized, double-blind, placebo-controlled, parallel-group, dosecomparison study conducted between April 2007 and October
2008. A total of 54 centers in the US randomized and reported
at least 1 patient with a gout flare. Overencapsulated (to
preserve double-blindedness) colchicine (USP 0.6-mg tablets
[Colcrys]) and matching overencapsulated (to preserve
double-blindedness) placebo were provided by URL Pharma.
A key aspect of the study design was that patients were
enrolled and were dispensed a double-blinded blister card of
study medication, at screening, prior to the onset of a gout
flare. Patients were required to call the Gout Flare Call Center
before taking study medication. This center was staffed 24
hours a day by medically trained personnel (e.g., nurses). Upon
clearance from the Gout Flare Call Center, patients were
PATIENTS AND METHODS
Characterization of colchicine pharmacokinetics.
Prior to the AGREE trial, the pharmacokinetics of low-dose
colchicine (1.2 mg followed by 0.6 mg in 1 hour [1.8 mg total]),
“high-dose” colchicine (1.2 mg followed by 0.6 mg every hour
for 6 hours [4.8 mg total]), and single-dose (0.6 mg) colchicine
were evaluated in healthy volunteers who had fasted. None of
these healthy volunteers participated in the AGREE trial.
Colchicine, United States Pharmacopeia (USP) 0.6-mg tablets
(Colcrys), was provided by URL Pharma (Philadelphia, PA).
Pharmacokinetic sampling occurred over 96 hours. Analytic
13